Equine Lameness Conditions

Equine Lameness Conditions
There are so many conditions that could be discussed in this section, I have chosen a few. On the website there are articles about other conditions that may have more detailed information. The ones that I included here are often the more frequently seen problems.
Foot Issues
The photographs below show the work of three different farriers working on three different horses in the same barn. Is one appoach better than another? Not necessarily, they all have similar goals in mind, but it is their approach that highlights the differences:



Lameness in the forefoot is by far the most common unsoundness in the horse. There are a multitude of reasons for this such as anatomy, shoeing and trimming methods and athletic activities. When one considers how small the horse‘s foot is relative to the body mass it is supporting just at rest, then add in the various forces that affect the foot with exercise it‘s remarkable that there are not more problems.
Anatomically the foot is a complex structure with bones that need to be in correct alignment. There are tendons and ligaments that insert into these bones and exert various forces depending on what action is being taken. Even at rest there are areas of tension. There are joint capsules and joint surfaces that are potential sites for inflammation when problems develop. Bursae, fluid filled structures that prevent irritation to a tendon as it passes over a bone, are located throughout the body. There is one bursa in each foot along the back edge of the navicular bone. As with joints these bursae can become inflamed. Other non-joint related tissues that can account for foot pain are the laminae or interconnected "fingers" that are responsible for maintaining the coffin bone in position along the hoof wall. A foot lameness may involve more than one of these structures at a single time.
For more information see the article on Foot Lameness located on this website. A thorough article evaluating horse’s feet and the use of horseshoes written by Dr. Stephen O’Grady at Northern Virginia Equine can be viewed here as well as other articles written by the farrier and Veterinarian who has a specialty equine podiatry practice: article by Dr. O’Grady.
Fetlock Disease

The fetlocks are commonly involved with equine lameness issues and examples of several problems are seen below. There are many soft tissue structures involved with the fetlock and when a problem is localized here it may need to be evaluated not only with digital x-rays, but also with ultrasound. The joint capsule, suspensory and sesamoidean ligaments are all intimately involved with the fetlock as are the flexor tendons and their tendon sheaths.

Swelling evident around an acutely injured fetlock, but no evidence of bone disease.

Bone fragment found in back of fetlock arising from the pastern.

Multiple areas of degeneration with calcification and proliferative reactions adjacent to the sesamoid bones and joint margins.
As with foot issues it's important to evaluate shoeing as hoof balance and proper support are essential when trying to resolve either an acute or chronic problem. Treatment options vary from topical sweats and anti-inflammatory preparations to intra-joint and/or systemic medications, laser and shockwave therapy. Often a combined approach is most successful.
Tendon and Ligament Disease
The term "bowed tendon" strikes fear into the heart of many a horse person as the potential for a long recovery and decreased performance is always a concern. Naturally not every tendon or ligament issue is disastrous, but once there have been disruptions in the fibers of these structures they will need treatment, rest and a period of physical therapy before a horse can return to full use. The lay-up could be several weeks and for some up to 6-12 months. The severe bow in the below image on the left would probably fall into the latter category. The second picture depicts a more diffuse swelling that may be what some of these severe bows may look like after they have reorganized. The green support wrap on the left leg is the type of support that may be used during recovery. In the picture on the right you can see a horse wearing a Sports Medicine Boot. These are easily applied and will provide a great deal of support when the horse is being exercised and may be recommended as the horse starts back into exercise.


Treatment options have advanced significantly even in the past 5 years. Early treatments involve icing and cold water therapy, topical cooling liniments and anti-inflammatories along with limited walking all depending on the results of an ultrasound exam. These early treatments are the mainstay for addressing an acute injury. Adding in ice boots and Game Ready Systems we can accelerate the cooling of these inflamed tissues more effectively. Shockwave and Laser Therapy, in my opinion, have been remarkably successful in this practice either separately or combined to reduce swelling, decrease inflammation, limit the formation of scar tissue and promote a faster, healthier healing pattern. The injection of "growth factors" into the damaged tissue with PRP and stem cells is undoubtedly one of the best ways to go to also promote a healthier tissue by supplying cells that can be used in the fiber healing. Stem cells can be acquired from a few sites on the horse's body or from fetal dental pulp tissue and PRP uses the horse's blood as the source. Treatment options are many and depending on the severity and the time frame they should be explored fully as it's essential that tendon and ligament function is restored as completely as possible.
Back and Neck Issues
Problems in these areas are not always as readily apparent as they are with lower limb problems that result in an obvious head bob or a hip hike. Often they may be considered by owners after dealing with a training issue, but they may have more of a primary role in causing a lameness, affecting the way a horse travels and explaining possible behavioral issues. Fortunately with a chiropractic exam and thorough limb and body palpation some of these concerns can be determined. The horse's spine is curved throughout the neck and back area and there needs to be the correct amount of flexibility and resistance to flex properly yet be able to carry the weight of the rider.
As can be seen from the picture below on the left there is a large amount of muscle along the top of the horse's back and neck. The more developed it becomes, the more a horse develops a muscular topline. Once a horse graduates to the appearance of the horse on the right - typically due to age and/or a less than regular exercise program -, the spine is being curved down and the supporting muscles below and above the vertebrae plus those along the lower abdominal wall have a loss in tone that results in this shape.

In the next set of images you can get a sense of some of the external to internal structures and the alignment with the spine curves I mentioned. The withers are made up of the dorsal processes of the thoracic vertebrae that extend up above the shoulder blade. The rider's weight is carried in the area where the back support is enhanced by its shape, the muscles and the rib cage.



The next 2 images give you a view looking down on to a horse’s back.


Once a horse graduates to the appearance of the horse below - typically due to age and/or a less than regular exercise program as the supporting topline muscles decrease - the spine is being curved down and the supporting muscles below and above the vertebrae plus those along the lower abdominal wall have a loss in tone that results in this shape.

The horse's spine and all the interconnected structures must function smoothly together, have flexibility and be able to carry the rider engaged in different disciplines. These are significant accomplishments and one of the reasons that spinal misalignment that results in chiropractic issues are frequently a consideration. I haven't even mentioned the role of a saddle and how improper fit can cause some of the chiropractic and muscular issues that at the very least can make a horse uncomfortable to ride.
I wouldn't suggest that every horse needs a chiropractic exam, but there are many primary and secondary issues associated with a horse's spine that develop over time. Chiropractic adjustments, acupuncture and mesotherapy are some of the alternative techniques that are used in this practice to work with these issues. Injections of medications into some of the affected structures, in and around kissing spines and/or intra-joint are common procedures along withe use of Shockwave and Laser Therapy. Digital x-rays, ultrasound and/or thermography are frequently used to aid diagnosis of some of these conditions.
Sacro-iliac Disease
Discomfort in the sacro-iliac area has been recognized as a cause of lameness and poor performance for some time, but in the past several years there has been more of a focus on it in the equine veterinary community. Exactly how to diagnose it and access the area has become a source for discussion that has led to disparate theories.
Part of the problem is that the region is hidden by a portion of the pelvis that limits our ability to recognize disease processes involving the joint and its associated ligaments. As you can see from the picture below the yellow indicates the wing of the pelvis that is the foundation of the hip area. The blue color indicates the sacral vertebrae. At the junction of the blue vertebrae with the pelvis on the underside of the yellow wing is shat makes the sacro-iliac joint. In addition to the joint there are ligaments that can be intimately involved with pain in this area and they are located above and below the pelvic wing. So if we decide there is pain in this area how do we know if we are dealing with just joint pain, ligament pain, muscular problems or sciatic nerve involvement ("sciatica") or even a combination of these structures? The answer is we often can't be sure. There are techniques such as Bone Scans that may help to answer these questions, but even that is limited.

If you are familiar with the term "hunter's bump" then you may have seen the result of problems with the sacro-iliac. When these bumps are recognized either as one or two the horse will have a visibly elevated bump on the top of the croup. They are best seen from behind, but in the middle horse from below, there is a definite rise and peak at the top of her pelvis. This area would indicate the presence of hunter's bumps. In order for these bumps to occur on one side or both there has to be some type of disruption of the articulation between the pelvis and the sacral vertebrae. It's possible for horses to live with these for years without incident, but in the acute phase this can cause a significant amount of discomfort.

Experience with palpation and joint motioning, used in chiropractic evaluations, is probably one of the most effective methods to recognize problems in this region. Treatments are many and it helps to determine whether we are dealing with a primary or secondary sacro-iliac problem. In the picture below I have been "motioning" the right side of the pelvis in an attempt to evaluate sacro-iliac range of motion and am preparing to adjust this area.

A horse with sacro-iliac pain may have shortening of the stride on the affected side, possibly appear lame, be reluctant to fully engage the hind end, drag a toe and/or refuse to comfortably canter. Of course these signs could be associated with other regions too. If a horse is definitely having a problem with this joint and its associated soft tissue structures then there will be limited motion either because the joint is "fixed" in position or because the horse is limiting motion in an attempt to protect the area through “splinting” of the muscles as full use might cause more discomfort. This would be analogous to one of us falling or slipping such that your sacro-iliac goes out. A number of things have been reported with people: localized pain, shooting pain down the leg, an altered way of walking and/or an acquired shortening of the leg on the affected side. Just the way our stride would change so could a horse's.
Once I determine that the sacro-iliac needs treatment a variety of methods have been used:
Chiropractic Adjustments
Acupuncture
Injections of anti-inflammatories (steroids) adjacent to sacro-iliac joints - done with ultrasound visualization to guide needles to the cranial and caudal sites
Mesotherapy
Shockwave Therapy
Laser Therapy
Some of these are done in combination and a period of prolonged physical therapy may follow as a horse resumes exercise. Treating these is not always straight forward and proper management before and after whatever methods are used is key to a successful outcome.
Hock Disease
Inflammation of the hock joints is a very common cause of hind end lameness, but certainly not the only one. Undoubtedly these joints are treated more frequently than other areas and I would argue they may be over medicated in the expectation that most hind end problems originate here. Further confusing the issue is whether more than one area - stifle, sacro-iliac or fetlock - is involved in a lameness and whether the origin of the suspensory ligament that attaches to the cannon bone just below the hock could be mimicking hock disease.
From the pictures below on the left you can see the classic picture of "bone spavin" as seen from the outside. This is looking from front to back and a bony proliferation is occurring on the inside of the left hind hock joint. The x-ray shows the site of degeneration in this hock. The line indicates the place where a joint space should be, instead there is fusion of the joint and a significant amount of bony reaction at this site. On the right picture you can see a needle with abnormal joint fluid dripping from the distal intertarsal hock joint. Normal joint fluid is clear, thick and yellow. Fluid with blood indicates inflammation and an injection with steroids into an affected joint will help to reduce inflammation.



Hind suspensory ligament disease is often a consideration with hock issues. It may be difficult to separate the two without blocking either the origin of the ligament or the hock joints. Unfortunately the confusion doesn't end there as one block might also affect the adjoining area. Ultrasound exams and x-rays are particularly useful in ruling in or ruling out these areas in addition to the blocks.
Traditional hock treatments involve intra-joint treatments, especially with steroids and Hyaluronic Acid. Systemic treatments with Legend and/or Adequan are also useful and for some horses, depending on the degree of degeneration and pain, anti-inflammatories such as Bute or Previcox/Equioxx may be needed for pain management.
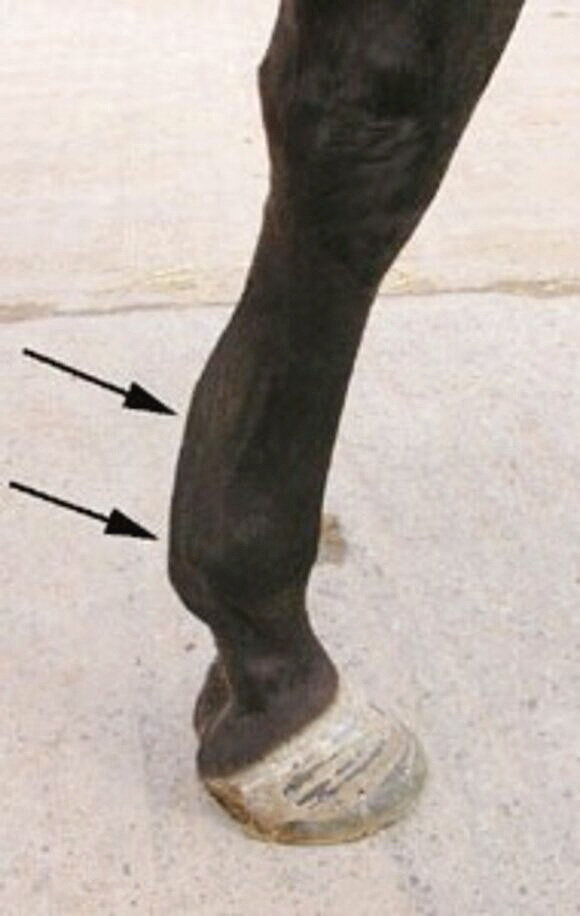
Distal Suspensory Ligament Disease (DSLD with Hind Fetlock Loss of Support)
Perhaps one of the most vexing lameness conditions that any of us will deal with involves degeneration of the Suspensory Ligament where a horse will lose support that results in over extension or dropping of the hind fetlock joint. As you can see from the pictures below as the support is lost the fetlock drops and the pastern starts to flatten out and can be parallel to the ground in more advanced cases. Once the degeneration starts, possibly before the dropping occurs, there will be a considerable amount of pain. This may be evident in how the horse walks or trots around, but it will especially be evident with palpation and flexion of the hind fetlock.
Once the joints are over-extended as seen in these pictures there is pain involving other areas of the joints and supporting soft tissues as they are not designed to be stretched in this fashion. Frequently swelling develops which over time hardens as the stressed soft start to change with respect to their normal elasticity. Eventually the fetlocks start to enlarge as is seen with the photo on the right.



There are no cures for this condition. Instead our efforts are geared towards helping support the area, ease breakover with improved trimming and shoeing and pain management. There was a study done in the previous years using Chinese herbs combined with another medication that has provided some encouraging results. I have used this protocol for a while and feel that it has significantly improved some of my patients. Still the management will require a multi-faceted approach, but with more options available to us plus help from the farriers there are some hopeful signs, still retirement may likely be in order.
